
Air Crescent Sign
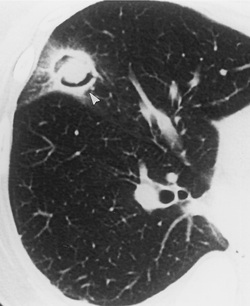
The air crescent sign can be visualized in a pulmonary cavitary process, which results in air surrounded by radiopaque material along both its inner and outer margins.
Despite being described in a number of entities, the air crescent sign is characteristic of invasive pulmonary aspergillosis when seen in the appropriate clinical setting. In this case, the hyphal form of the fungus invades the pulmonary vasculature resulting in pulmonary hemorrhage, arterial thrombosis, and eventual infarction. Over time, with retraction of the infarcted center and peripheral reabsorption of necrotic tissue by leukocytes, a central area of devitalized tissue is formed. The air crescent sign results when air fills the space between the devitalized tissue and surrounding parenchyma. An opaque rim of hemorrhagic tissue peripheral to the radiolucency makes visualization of the air crescent possible.
The pathologic basis for an air crescent sign in invasive aspergillosis may be shared with other angioinvasive fungal infections or bland thromboembolism. A cavitating neoplasm, infections such as tuberculosis, nocardiosis, or a bacterial lung abscess may also give rise to an air crescent sign. Also seen in pulmonary haematoma, benign & malignant lung tumours, granulomatous disease, Rasmussen’s aneurysm.
Despite being described in a number of entities, the air crescent sign is characteristic of invasive pulmonary aspergillosis when seen in the appropriate clinical setting. In this case, the hyphal form of the fungus invades the pulmonary vasculature resulting in pulmonary hemorrhage, arterial thrombosis, and eventual infarction. Over time, with retraction of the infarcted center and peripheral reabsorption of necrotic tissue by leukocytes, a central area of devitalized tissue is formed. The air crescent sign results when air fills the space between the devitalized tissue and surrounding parenchyma. An opaque rim of hemorrhagic tissue peripheral to the radiolucency makes visualization of the air crescent possible.
The pathologic basis for an air crescent sign in invasive aspergillosis may be shared with other angioinvasive fungal infections or bland thromboembolism. A cavitating neoplasm, infections such as tuberculosis, nocardiosis, or a bacterial lung abscess may also give rise to an air crescent sign. Also seen in pulmonary haematoma, benign & malignant lung tumours, granulomatous disease, Rasmussen’s aneurysm.
